
Lateral Ligament Repair
Surgery to Repair Ankle Ligaments
The diagnosis of ‘sprain’ literally means a ligament injury. Whilst most of us have probably suffered an ankle sprain at some point in our lives, the vast majority of these will recover without the need for surgery. Most simple ankle sprains will heal naturally over the course of a few weeks. More serious sprains may require physiotherapy and can take several months to recover. Whilst physiotherapy will help most achieve recovery, some patients experience continuing problems and these patients can be helped by daycase surgery using modern keyhole techniques.
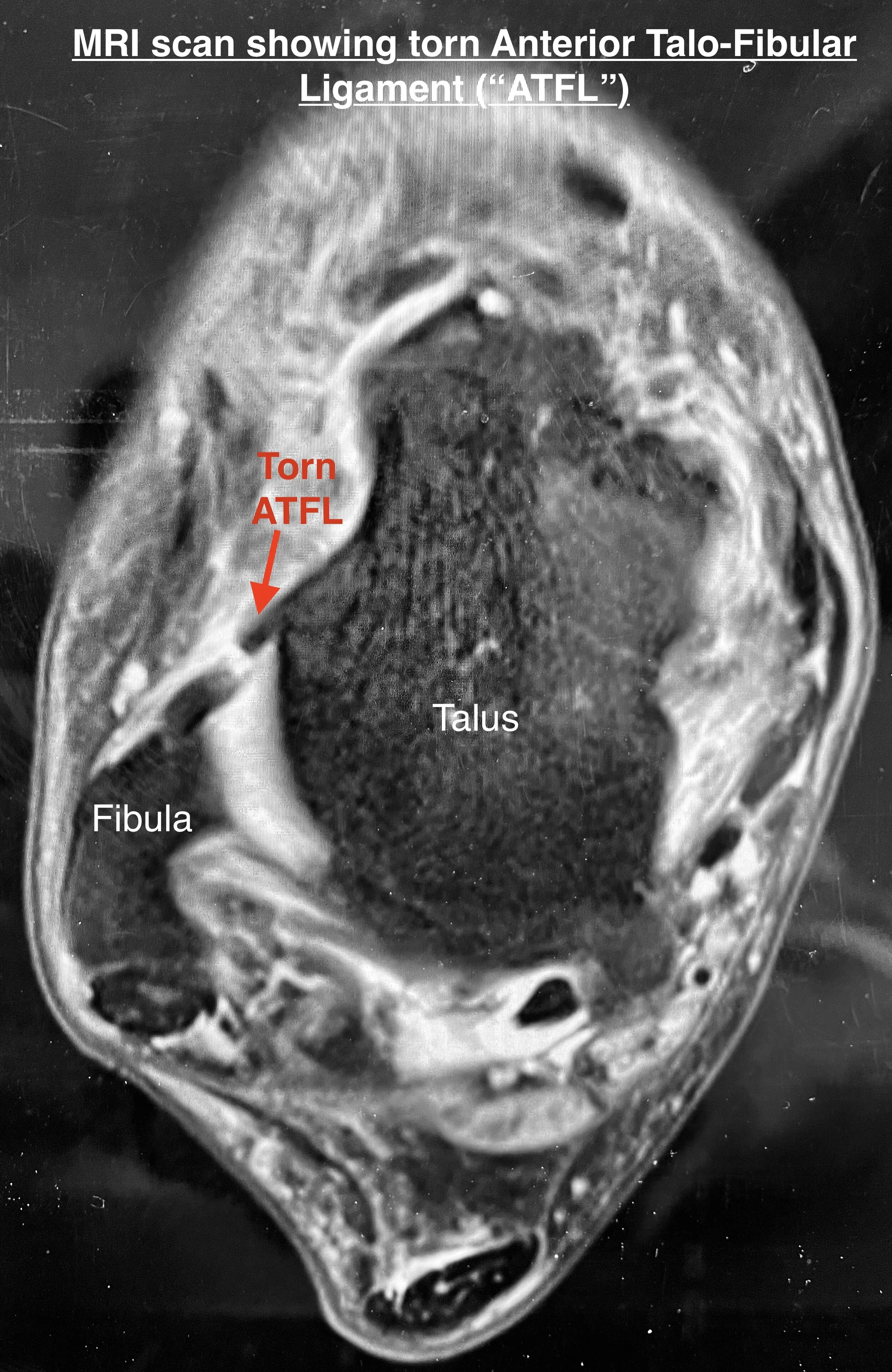
MRI scan
An MRI scan is very useful in confirming torn or damaged ligaments in the ankle and is also important to ensure that there is no other damage to the nearby tendons or the ankle joint.
This image shows a cross section of the ankle on MRI and the torn anterior talofibular ligament can be clearly seen. This is the most commonly injured of the ankle ligaments and failure of this ligament to heal properly can lead to symptoms of instability (ankle giving way or rolling over easily) and/or insecurity (not trusting the ankle).
Sometimes the patient will also complain of pain in the ankle due to inflammation inside the joint (called synovitis). This can sometimes result from the lack of constraint of the joint which allows the lining of the joint to be ‘pinched’.
Alternatives to surgery:
• Accept level of symptoms and limit activity to control these symptoms
• Wear an ankle foot orthosis (AFO “brace”) to stabilise ankle
• Physiotherapy treatment will usually have been tried before discussing surgery
Main Risks Of Surgery:
Swelling/Scar -Initially the foot and ankle will be swollen and needs
elevating. The swelling will disperse over the following weeks and months
but will remain evident for up to 3-6 months. The scar can cause irritation
to begin with but usually settles to a great extent over the first 4-6 weeks.
Wound healing problems - The risk of serious wound healing
problems is approximately 1%. It is important to keep the foot elevated
over the first 10 days to reduce the swelling and risk of wound healing
problems. In rare circumstances when the wound is problematic, further
surgery can sometimes be required.
Infection -The risk of deep infection occurring is approximately 1%. You
will be given intravenous antibiotics to help prevent this. It is important to
keep the foot elevated over the first 10 days to reduce the swelling and risk of
infection. If there is an infection, it may resolve with a course of antibiotics
but may require a period of hospitalisation or rarely, further surgery.
Nerve damage -The superficial peroneal nerve is close to the
incision. This supplies sensation to the top surface of the foot. This may
rarely (1%) be damaged during the surgery and this may leave a patch of
numbness on the top surface of the foot. This numbness may be
permanent would not affect function.
Main Risks Of Surgery Cont...
Re-rupture of the Ligaments - Following surgical repair of
the ligaments there is no evidence to suggest that you are at higher risk of
repeat injury to them but in some cases the shape of the hindfoot can
predispose you to ankle sprains and this will be discussed pre-operatively
as very occasionally further surgery can be advised to try and reduce this
risk. It is very important that patients follow the post operative instructions
provided to minimise the risk of further problems.
Deep Vein Thrombosis (DVT) - This is a clot of blood in the
deep veins of the leg. The risk of a clot occurring is reported as less than 1%
after foot and ankle surgery which is generally substantially lower than after hip
or knee surgery. Suspicion of DVT is raised if the leg becomes very swollen
and painful. There are tests that can be performed to confirm / exclude the
presence of a DVT. If confirmed, you will probably require treatment with a
blood thinning agent (heparin preparation and / or warfarin). The main concern
with regards a DVT is that rarely (<1:1000 chance with foot and ankle surgery)
a piece of clot can break away in the leg and travel to the lungs which is much
more serious and can be life-threatening. This is called a pulmonary embolus
and signs of this include chest pain and shortness of breath.
For the first 2 weeks following surgery it is likely that you will be treated
with a blood thinning agent (LMWH - low molecular weight heparin
injections) to minimise the risk of DVT / PE but this does not afford total
protection and exercises to keep the toes and knee moving are advised, as
well as remaining generally mobile.
If you are concerned that the leg has become more swollen and painful
(some swelling always occurs after surgery), or if you experience chest
pain / shortness of breath, then you should contact the hospital, general
practitioner, or accident and emergency department immediately.
Sick Leave
In general 4 weeks off work is required for sedentary employment, 12
weeks for standing or walking work and 16 weeks for manual / labour
intensive work. We will provide a sick certificate for the first 2 weeks;
further certificates can be obtained from your GP.
Driving
Usually you may return to driving after outpatient review at 2 weeks
These notes are intended as a guide and some of the details may vary
according to your individual surgery or because of special instructions
from your surgeon.
Lateral Ligament Reconstruction
Post-Operative Course
Day 1
• Below knee cast (backslab plaster) applied at end of surgery
• Expect some numbness in foot for 12-24 hours
• Pain medication and elevation of foot
• Blood drainage through cast expected
• Mobilisation non-weight bearing with physiotherapist (crutches)
• No weight through operated leg for 3 weeks
• Treatment with LMWH injections
• Discharge home usually possible on day of surgery (otherwise overnight stay)
• May shower / bath if able to keep leg dry
2 Weeks
• Outpatient review of wounds (and removal stitches if necessary)
• Cast replaced with stirrup splint
• No weight bearing on operated leg until 3 weeks post surgery
• Patient to remain in stirrup at all times (day and night)
• Supervised and unsupervised physiotherapy may begin. Only include:
• Swelling control - ice, elevation, effleurage and massage as appropriate
• Scar mobilisation
• Gentle active exercises until 3 weeks post surgery
• Usually you may return to driving after outpatient review at 2 weeks
3 Weeks
• May begin full weight-bearing in stirrup splint
• Stirrup splint to be worn until 10 weeks post surgery
• Physiotherapy to continue as instructed by physiotherapist including:
• Regime as for an acute lateral ligament sprain
10-12 weeks onwards
• Outpatient review
• Physiotherapy to continue:
• Re-introduce sport (consider AFO for further 4 weeks during sport)