
Keyhole surgery for hallux rigidus (Big Toe Arthritis)
Minimally Invasive Cheilectomy
Minimally Invasive Cheilectomy Surgery
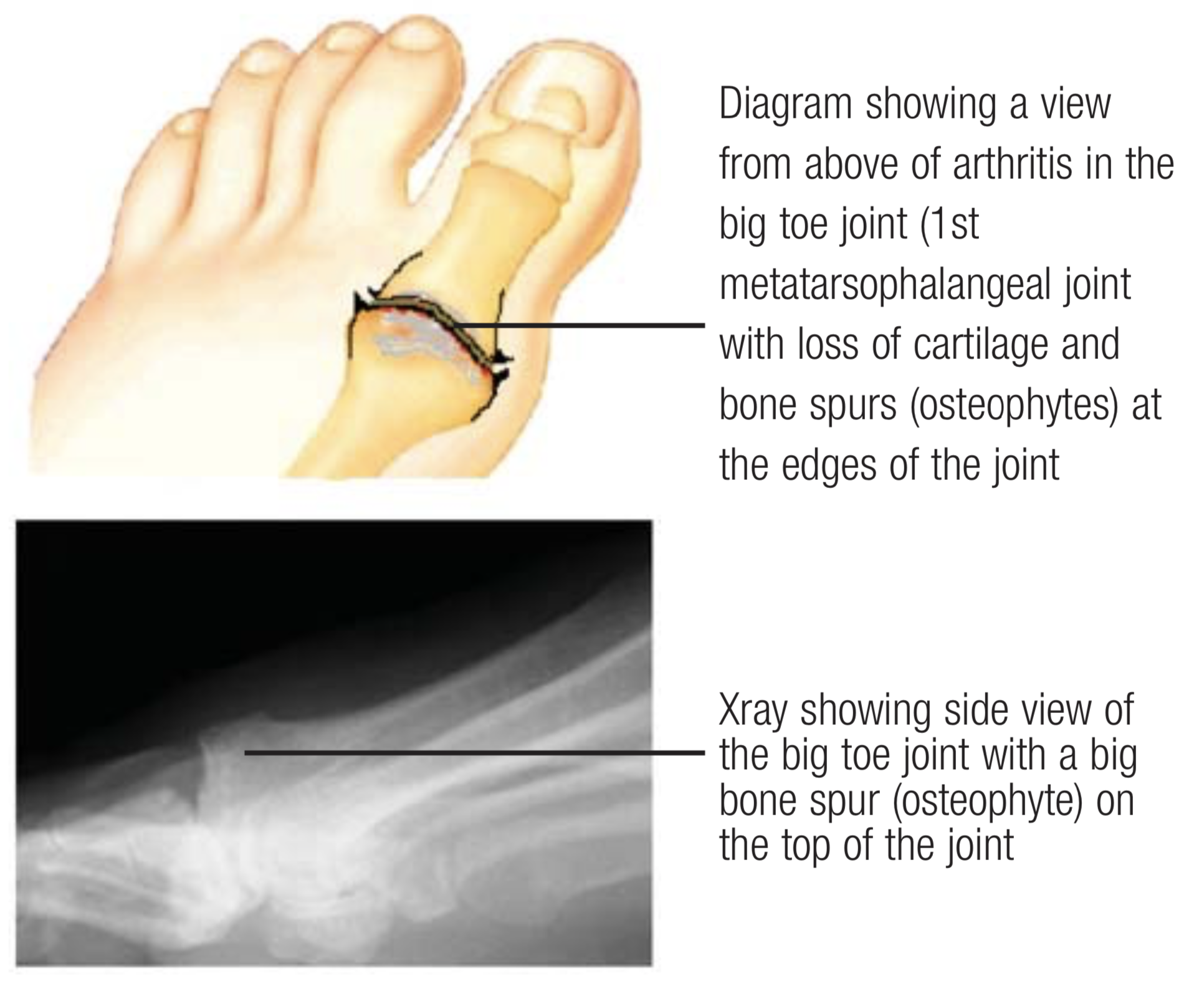
Hallux Rigidus refers to stiffness in the big toe joint (1st metatarsophalangeal joint) due to ‘wear and tear’ osteoarthritis. There is often a family history and if one big toe is affected then it is very likely that the other will be too at some point.
Movement of the big toe joint occurs in an up and down plane only (dorsiflexion and plantar flexion). The normal upward movement (dorsiflexion) is approximately 90 degrees, and the normal downward movement (plantar flexion) is 25 degrees.

Click to see medical section article about Mr Redfern’s keyhole surgery for hallux rigidus
Mr Redfern receiving the 2019 European Award in Orthopaedic Surgery for his innovative state of the art techniques
Treatment of hallux rigidus often requires surgery but the joint can be made more comfortable without surgery by careful choice of shoes (eg. stiff soled and rocker bottom), modifying shoes, orthotic supports inside the shoes, and analgesics (pain killers). In general, the thinner the shoe sole, and the higher the heel, the worse the symptoms from this condition due to stress on the big toe joint, which increases pain. A steroid injection can sometimes also be helpful as a temporary measure to control painful symptoms and Mr Redfern will be able to discuss this with you.
The surgical treatment for hallux rigidus is determined by the extent of the arthritis in the big toe joint (metatarsophalangeal joint).
Hallux Rigidus
Arthritis in the big toe joint often causes pain and stiffness in the joint.No treatment is required unless the pain is intrusive.
If non-operative treatments are not sufficient then there are very effective surgical options. State-of-the-art modern keyhole surgery techniques, pioneered in the UK by Mr Redfern, can be helpful to ‘tidy up’ spurs and ridges of bone from the joint which are often responsible for pain and restriction in joint movement.
Minimally Invasive Cheilectomy
This operation is aimed at treating a stiff painful big toe joint in which arthritis has developed. As a result of the arthritis, there is limited upward (dorsiflexion) movement of the big toe. The operation helps improve painful symptoms as the big toe bends upward by removing the spurs that block joint movement.
In addition to the improvement in pain, some improvement in movement of the toe is also usually achieved - although this varies due to the arthritic process in the joint. The key to a successful operation is to begin bending the big toe soon. As soon as pain permits, you need to start bending the big toe upwards and you will be shown how to do this by a physiotherapist while in the hospital immediately after the operation.


Because the underlying condition is due to arthritis of the big toe, the final outcome will depend upon the further development of arthritis.
The name cheilectomy stems from the Greek word cheilos meaning lips, denoting the bony lips that grow on the top of the joint, causing the stiffness and responsible for most of the pain. The operation removes these obstructing lips and is sometimes combined with an additional cut in the bone at the base of the big toe to slightly shorten it, decompress the joint and gain a little more motion in the joint.
The traditional open operation is performed through a 5 cm incision on the top of the joint but Mr Redfern performs this surgery through an incision of less than 1cm on the inside border of the foot by using tiny instrument called burrs to remove the bone under hi-tech X-ray guidance.

Minimally Invasive Cheilectomy
Thus type of surgery relies on tiny instruments that are used to carry out the surgery under X-ray guidance - “eyes inside the foot”
Mr Redfern has trained the majority of surgeons offering this type of surgery in the UK and continues to travel worldwide training and lecturing in this field.
Video of a patient 1 week after Mr Redfern’s minimally invasive cheilectomy …




The operation is most successful if the arthritis is in the early stages. Approximately 80-85% of patients are satisfied or very satisfied with the results of this surgery in the early stages of arthritis. If more advanced arthritis is diagnosed then Mr Redfern may still recommend a minimally invasive cheilectomy depending on your assessment but he may also discuss other surgical options such as osteotomy, fusion or a Cartiva implant.

Arthroscopy
Sometimes Mr Redfern will combine minimally invasive cheilectomy with arthroscopy of the joint
Sometimes Mr Redfern will recommend that the MIS cheilectomy is combined with an arthroscopy of the joint. An arthroscopy involves using a keyhole camera to look inside the the joint and this allows removal of any inflamed lining of the joint and further tidying of the arthritic joint using other mini instrument. If Mr Redfern advises this additional surgery then he will perform it at the same time as the cheilectomy and will usually make an additional keyhole at he level of the joint.
Following surgery, the toe is protected in a small bandage and post operative shoe. With Mr Redfern’s keyhole technique, you can take full weight on the foot immediately after surgery. You can also remove the bandages yourself at home the next day to simply leave a small dressing in place over the keyhole incision.
Elevation of the foot (above the hip) for the first 4 days is important to minimise swelling and help prevent infection.
The surgical shoe is worn for 4-7 days (moving into your own shoes from day 4 onwards depending on comfort)
General Recovery Facts
Operation performed under general anaesthetic (or regional anaesthetic)
You are able to walk on the foot immediately after surgery
You will be given a surgical shoe (flat shoe) to wear for the first few days after surgery
You may not drive after the surgery for at least 1 week unless you have an automatic vehicle and only the left foot has been operated on
The surgical shoe is worn for 4-7 days (moving into your own shoes from day 4 onwards depending on comfort)
Mr Redfern strongly recommends that you do not play sport or run for the first 4 weeks after surgery as this can aggravate the joint
Whilst for some patients there is very rapid relief of symptoms, for others it can take longer to see an improvement and it takes up to a year to assess the final result.
Approximately 80-85% of patients feel satisfied or very satisfied with the results of this surgery. Not all patients are suitable for this operation and Mr Redfern will discuss this with you
Post-operative Course:
Minimally invasive cheilectomy (+/- arthroscopy)
Day 1
Foot wrapped in bandage and surgical shoe worn
Start walking immediately in surgical shoe
Begin exercises to move the big toe immediately after surgery
Elevate foot above hip
Expect numbness in foot for 12-24 hours
Usually very little pain
Day 2
Remove bandages to leave small dressing in place
Continue elevation until day 5
Continue use of surgical shoe until day 5
Continue to maintain movement in the big toe
Usually very little pain
Day 5-7
From day 5, elevation only required sufficient to avoid swelling in the operated foot
From day 5, you can begin to wear your own shoes (eg trainer) as comfort allows
Outpatient review by Mr Redfern usually at 7 days after surgery (incision inspected and stitches removed if used)
Shower when incision dry
Usually very little pain
After 1week review
Physiotherapy often advised to help optimise big toe movement and restore gait
A regular shoe may be worn if comfortable
No sports for 4 weeks after surgery
Return to activity as guided by comfort
No high heels to be worn for three months after surgery
Can take up to a year to assess final result but most of those patients who are going to respond well to the surgery will feel an improvement within the first 6 months
An image-guided steroid injection can be helpful sometimes if progress is slow and Mr Redfern can discuss this with you if necessary
Main Risks of Surgery:
Minimally invasive cheilectomy
Infection – This is an extremely small risk with this type of surgery. In Mr Redfern’s practice the risk is less than 1% across all of his keyhole surgery. Even though infection is rare, it is important to maintain elevation of the foot after surgery as instructed to minimise this risk.
Wound problems – Occasionally the small incisions can be slower to heal and this does not usually cause a problem but needs to be closely observed for any infection occurring.
Nerve Injury – The risk of the small nerves in the area being directly injured by the surgeon is approximately 1%. However, the nerves can become bruised by the surgery as a result of the swelling (10%). Whilst this usually recovers, you could end up with some permanent numbness over the big toe area, which might cause irritation.
CRPS – This stands for complex regional pain syndrome. It occurs very rarely in Mr Redfern’s practice (<1%) and is not properly understood. It is thought to be inflammation of the nerves in the foot and it can also follow an injury. We do not know why it occurs. It causes swelling, sensitivity of the skin, stiffness and pain. It is treatable but in its more severe form can takes many months to recover.
Deep Vein Thrombosis (DVT) – This is a clot in the deep veins of the leg and the risk of this occurring following foot and ankle surgery is low (generally< 1%). However, because Mr Redfern does not need a tourniquet on the leg for the keyhole cheilectomy, the blood flow is not interrupted during the surgery. This, combined with the immediate full weight bearing mean that the risk of DVT is extremely rare - Mr Redfern has not seen a DVT after minimally invasive cheilectomy in over 10 years of performing this operation. However, it is probably sensible to avoid a long-haul flight in the first 4 weeks following surgery.
If a deep vein thrombosis (DVT) occurs then you will require treatment with heparin and Warfarin to try and prevent any of the clot travelling to the lungs (pulmonary embolus / PE) which can be much more serious).
Continuing symptoms– Most people (80-85%) are very happy with the results of their cheilectomy surgery but you can appreciate that if some of the above problems occur then this may also affect the end result. If the toe joint remains stiff and painful despite this surgery then other surgical options may need to be discussed such as osteotomies, Cartiva or fusion.
Sick Leave
In general 1 week off work is required for sedentary employment, 2-6 weeks for work involving standing or walking, and 4-6 weeks for manual labour work.
Driving
Generally, most patients will return to driving a manual car at one week after surgery although, if it is only the left foot that has undergone surgery then return to driving an automatic vehicle is allowed after 48 hours.