
Ankle Arthroplasty
Total Ankle Replacement
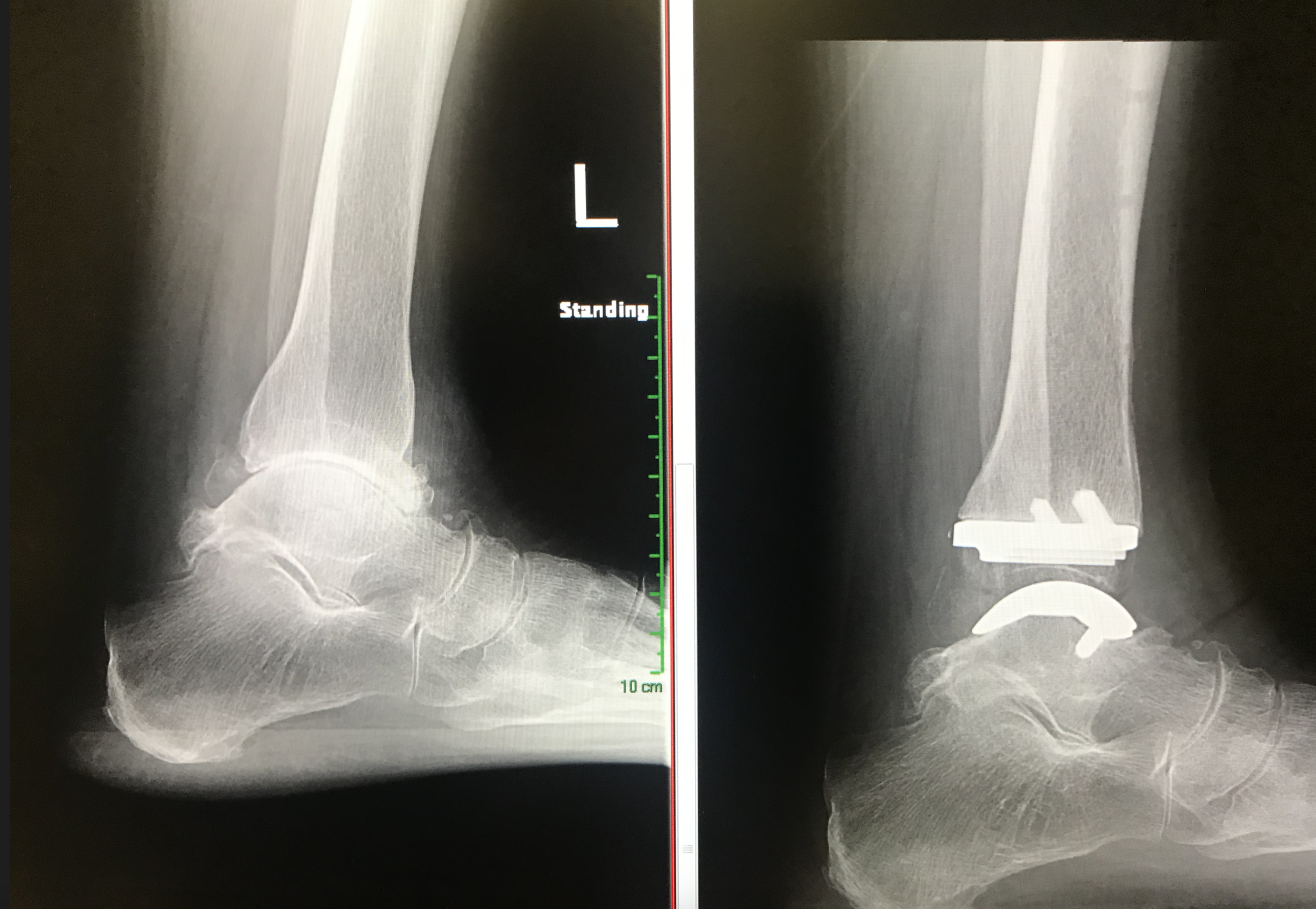
Total Ankle Replacements: Infinity Implants
This operation replaces the painful arthritic ankle joint with an artificial metal and polyethylene joint.
The joint will remain mobile and ideally painfree. Following surgery, you should be able to walk normally, with much less pain or painfree.
Motion in the ankle joint is usually at least as good as before surgery (unlikely to be very much more range movement than prior to surgery)

Infinity Total Ankle Replacement
This implant is made by Wright Medical USA and involves replacing the bony surfaces on both sides of the joint with metal bearings. The polyethylene spacer is attached to the tibial bearing but free to articulate with the talus bearing.

Learn about a patients experience with the infinity ankle replacement here http://www.myankle.com/johnny-b/. Individual patient results vary and only an orthopaedic surgeon such as Mr Redfern can determine the best course of treatment for you. Many factors contribute to the length of hospital stay and rehabilitation.
Modern designs of ankle replacement have not yet been in use for sufficiently many years for there to be good quality information on long term outcome (unlike hip and knee replacement) but short term data is encouraging. In view of this Mr Redfern will inform patients that this type of surgery has to be considered experimental although hundreds of these ankle replacements have been implanted worldwide.
Mr Redfern has been performing ankle replacement surgery for 20 years now and has experience with several different implants as well as experience in looking after complex patients who require staged surgery or further surgery including complex conversion to ankle fusion.
In other words, whilst we expect the design to perform well in the longterm, we do not yet have data to confirm that this is the case and hence it is sensible to expect that further surgery such as an ankle fusion might be required sometime in the future if / when the implant needs to be removed (in the event that it becomes problematic and no longer functioning correctly).
An alternative surgical option is to consider ankle fusion. This option will be discussed with patients and the pros and cons of the two operations discussed.
The surgery is performed through an incision of approximately 15 cm over the front of the ankle. The arthritic joint surfaces are excised (cut out) and the tibia and talus shaped to receive the new joint components. The implants are locked in place and without the need for bone cement (the bone grows into the special surfaces on them). The operation takes approximately 2 hours.

Infinity Ankle
Infinity ankle replacement shown in a model skeleton. The implants replace both tibia and talus articular surfaces and have a high density polyethylene articulating spacer between the two metal surfaces.
After surgery, your leg will be immobilised in a backslab (half plaster) for 2 weeks during which time you will not be allowed to take weight through it (crutches/scooter/frame used). Elevation of the foot (above the hip) over the first 14 days is vitally important to help prevent infection and assist with wound healing.
After 2 weeks the backslab will be removed in the outpatient department and the stitches take out. If all is well, you can begin weight bearing at that stage in a removable boot for a further 4 weeks with the aid of crutches.
General Recovery Facts:
You will not be able to walk on the leg for the first 2 weeks (leg in backstab cast)
After the first 2 weeks, four more weeks of restricted weight bearing in a removable boot
You will not usually be able to drive for the first 2 months following surgery (see below)
Ankle motion exercises begin at 2 weeks post surgery (including use of hydrotherapy if possible)
There will be moderate swelling of the ankle for approximately 6 months following surgery
There will sometimes be some aching discomfort in the ankle for up to 12 months following the surgery
The aim is to return the patient to an active lifestyle, including leisure walking, cycling, gymn, swimming and golf. It is not recommended that you run or undertake impact sports (skiing may be possible in some circumstances)



Post Operative Course: Total Ankle Replacement
Day 1
Ankle will be in plaster of Paris cast (below the knee)
You will have the leg elevated in bed
Whilst immobile in bed you will be given daily heparin injections to reduce the risk of a thrombosis (clot in the leg)
Blood drainage through the cast or bandaging is expected
The pain is controlled with various intravenous pain killers
Days 2 -3
The pain usually settles over the first few days
Whilst immobile in bed you will be given daily heparin injections to reduce the risk of a thrombosis (clot in the leg)
Postoperative x-rays may be taken
No weight through the operated limb (non-weight bearing)
Mobilisation with physiotherapist (crutches/frame/scooter)
Usually discharged from hospital after approximately 2-3 days once safe
At home keep the operated leg elevated most of time (above level of pelvis)
Do not interfere with the cast or dressings*
Keep the cast / dressings dry
2 Weeks
Outpatient department review for wound review & removal stitches
A removable boot is then applied (or sometimes a new cast)
Instructed to begin movement out of the boot 3 times a day ((physiotherapy begins)
Begin weight bearing on operated leg in the boot
You can shower / bath once wound healed (usually by 2 weeks post surgery)
6 Weeks
Further review in outpatient department with x-ray on arrival
Begin full weight bearing out of boot
Continue physiotherapy
Further outpatient review at 3, 6 and 12 months and yearly thereafter.
*if concerned then contact the hospital who can speak to Mr Redfern’s team.
Sick Leave
In general 6 weeks off work is required for sedentary posts, 12 weeks for standing or walking posts and 16 weeks for manual / labour intensive posts. We will provide a sick certificate for the first 2 weeks; further certificates can be obtained from your GP.
Driving
May return to driving after outpatient review at 2 weeks post surgery ONLY IF left leg surgery only and automatic vehicle – otherwise unable to drive until 2 months post surgery. Otherwise, in most instances, it is possible to return to driving at 2 months following surgery but this really depends upon comfort and an individual’s progress.
Main Risks of Surgery: Ankle Replacement
Swelling - Initially the foot will be swollen and will need elevating. The swelling will disperse over the following weeks and months but will remain evident for up to 6-9 months.
Infection – The risk of deep infection occurring is approximately 1-2%. You will be given intravenous antibiotics at the time of surgery to help prevent this. It is important to keep the foot elevated over the first 14 days to reduce the swelling and the risk of infection. If there is an infection, it may resolve with a course of antibiotics but may rarely result in the need to temporarily or permanently remove all of the implants.
Wound Problems – Wounds in this area of the body are very fragile and healing can be problematic on occasions. If this occurs then the risk of infection increases and this is a serious problem. Rarely (<1%), such wound problems can require plastic surgery to achieve healing and hence prolonged recovery.
Bleeding - Mr Redfern usually performs this surgery under tourniquet (a tight band on the thigh to prevent bleeding) and so there is rarely any significant bleeding at the time of surgery. There can often be some blood seeping into the plaster and bandages after the surgery. This rarely requires more than observation and blood transfusion would be extremely rare (risk <1%).
Nerve damage – There are several nerves crossing the ankle to supply sensation to the ankle and foot as well as controlling muscles in the foot. Despite great care in handling the tissues very delicately, small sensory nerves can be damaged during the surgery and this may leave a patch of numbness in the area of the incision of beyond this. This numbness may be temporary or permanent. There is approximately a 5% risk of this happening. The risk of suffering a nerve injury affecting the muscle function in the foot is <1% in Mr Redfern’s practice.
CRPS - This stands for complex regional pain syndrome. It occurs rarely in severe form and is not properly understood (risk <1% in Mr Redfern’s practice). It is thought to be inflammation of the nerves in the foot and it can also follow an injury. We do not fully understand why it occurs. It causes swelling, sensitivity of the skin, stiffness and pain. It is treatable but in its more severe form can takes many months to recover and can leave persisting pain and sensitivity.
Fracture - Because of the nature of ankle replacement surgery and the relatively small bones of the ankle (compared to the knee for example) there is a risk of the bones fracturing. This can happen at the time of surgery, in which case it will be fixed with additional metalwork if required. Fractures can also happen after the surgery during the recovery, and this may require further surgery depending on the type of fracture.
Mal-position – Ideally, the surgery is performed so that the implants are in the optimal position for function of the joint. Mr Redfern takes great care to judge the best position during surgery and the modern instrumentation is generally very reliable and reproducible in this respect but anatomy can still vary especially if there is a history of trauma or previous surgery in the past and it is not always possible to achieve ideal alignment (risk approximately 5%). If the position is not optimal during surgery, then additional re-alignment of the heel bone may carried out to improve this at the time. Rarely, further surgery required at a later date to address any remaining alignment concerns.
(Premature) failure of the replacement – the metal / polyethylene joint has an unknown lifespan at present but left long enough, all joint replacements will eventually fail. When it fails, it is sometimes due to subtle infection which can loosen the components or wear of the components (usually the polyethylene). This usually takes several years; we do not have an average lifespan for the replacements yet. Once the joint wears out, further surgery is normally required to fuse the joint together. Hopefully, this never becomes necessary, but a 10-15 year period is a reasonable estimate for the expected survival of the ankle joint although this is not guaranteed and some patients will require further surgery much earlier.
Dislocation – this is very rare and would require relocation of the joint under anaesthetic. It usually reflects an underlying problem with the joint that may require further surgery.
Amputation - This is fortunately very rarely required after such surgery. Whilst Mr Redfern has never had to resort to amputation following this type of surgery, the risk reported in the medical literature is approximately 0.5-2.5%. Overwhelming infection might be a reason to consider this which is thankfully rare.
Continuing pain - Despite the majority of patients reporting satisfaction with this type of surgery, some will have continuing pain or problems with the replacement joint that necessitate further surgery to remove the implants prematurely and convert to an ankle fusion. Generally, approximately 80-85% of patients report satisfaction with joint replacement surgery.
Deep Vein Thrombosis (DVT) - This is a clot of blood in the deep veins of the leg. The risk of a clot occurring is reported as <1% after foot and ankle surgery which is generally substantially lower than after hip or knee surgery. Suspicion of DVT is raised if the leg becomes very swollen and painful. There are tests that can be performed to confirm / exclude the presence of a DVT. If confirmed, you will probably require treatment with a blood thinning agent (heparin preparation and / or warfarin or similar drug such as Rivaroxaban). The main concern with regards a DVT is that rarely (<1:1000 chance with foot and ankle surgery) a piece of clot can break away in the leg and travel to the lungs which is much more serious and can be life-threatening. This is called a pulmonary embolus and signs of this include chest pain and shortness of breath.
Whilst in hospital following surgery it is likely that you will be treated with a blood thinning agent (LMWH - low molecular weight heparin injections) to minimise the risk of DVT/PE but this does not afford total protection and exercises to keep the toes and knee moving are advised, as well as remaining generally mobile. You are also likely be fitted for a compression stocking to be worn on the unoperated leg after surgery.
Once you have left hospital but remain non weight-bearing on the operated leg, you will probably require treatment with a blood thinning agent (low molecular weight heparin injections or oral drugs such as Rivaroxaban or Aspirin). Mr Redfern or his team will discuss this with you whilst you are in hospital.
If you are concerned that the leg has become more swollen and painful (some swelling always occurs after surgery), or if you experience chest pain/shortness of breath, then you should contact Mr Redfern’s team at the hospital, your general practitioner, or the accident and emergency department immediately.
